
The Society of Hospital Medicine and Choosing Wisely recommends reducing the frequency of daily unnecessary phlebotomy. We examined the lab ordering practices of 29 hospitalists and presented personalized data via the Agathos platform.
CONTEXT
Frequent blood draws can have negative consequences for hospital patients, from discomfort and poor sleep to anemia and increased risk of infection. While blood tests are an important part of the diagnosis and monitoring of hospital inpatients, excess ordering should be avoided. Ordering lab tests on recurring schedules is one practice that can contribute to unnecessary testing. Recurring labs can persist until cancelled and, if overlooked, may follow a patient throughout their stay despite previously stable results.
ANALYSIS
Choosing Wisely recommendations focus on two main types of lab tests: complete blood counts (CBCs) and blood chemistry (i.e., metabolic panels). At the 800+ bed hospital in this investigation, more than 97% of all inpatients had both a CBC and a metabolic panel, and over a third of those patients had multiple of these tests performed during their stay. Over 12 weeks, 16,555 total combined CBCs and metabolic panels were performed for any patient while one of the 29 hospitalists was the attending physician, which projects to approximately 72,000 tests in a year.
DAILY LABS
In order to focus on practices which contribute to unnecessary lab tests, we examined the number of CBCs and metabolic panels ordered on a recurring daily schedule. Scheduling labs once per day is typically done for convenience rather than clinical indication. However, more frequent recurring labs, such as every 2 or 4 hours, are generally placed for patients in more critical conditions and, thus, were excluded from the focus.
ATTRIBUTION
Daily labs are often placed toward the beginning of a hospital encounter, following the patient across department transfers and handoffs until discharge. Thus, two practices contribute to the persistence of daily recurring labs:
1. Ordering labs on a recurring daily schedule
2. Not cancelling existing daily lab orders upon receiving a patient hand-off
To capture these two actions for each of our 29 hospitalists, we counted the number of daily scheduled CBCs and metabolic panels performed while they were the attending on a stay. Some of these lab orders were placed directly by the attending hospitalist, and some had been placed by previous attending providers. Final data were calculated for each hospitalist as follows:
% labs as daily (in a category) = ( # of daily labs) ÷ (# of total labs)
FINDINGS
The data sent to one of the 29 physicians is shown below:
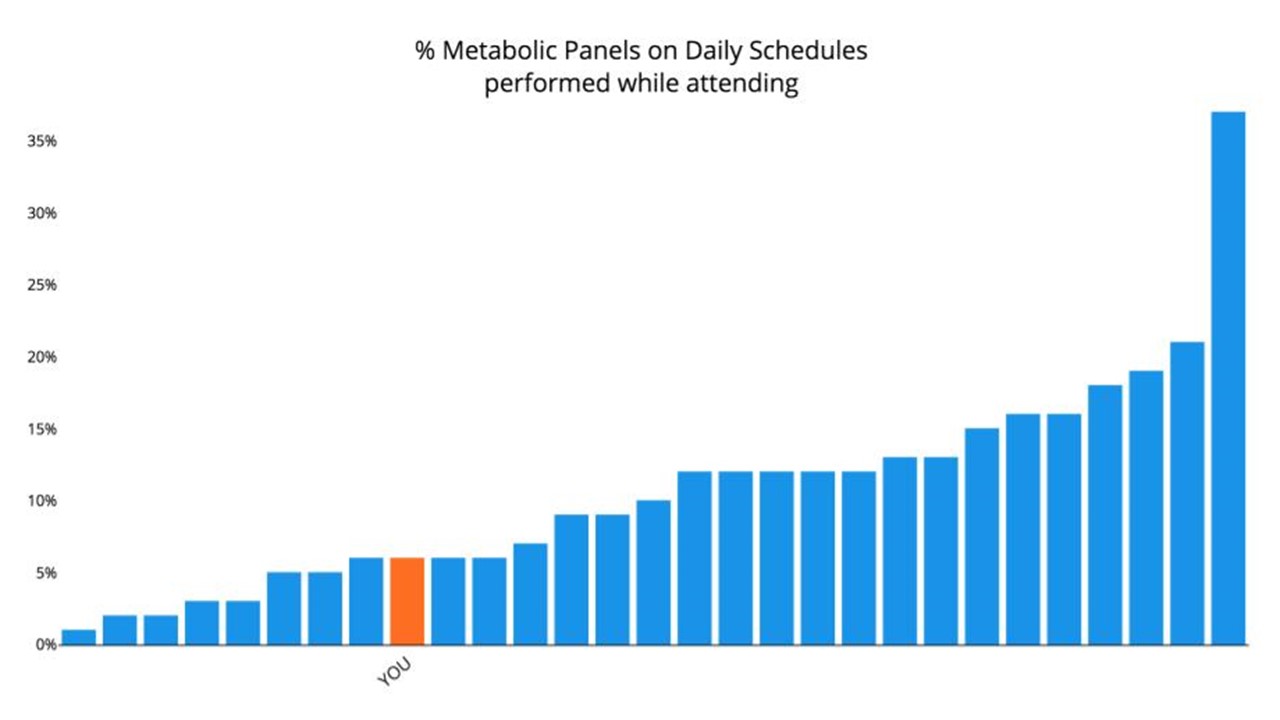
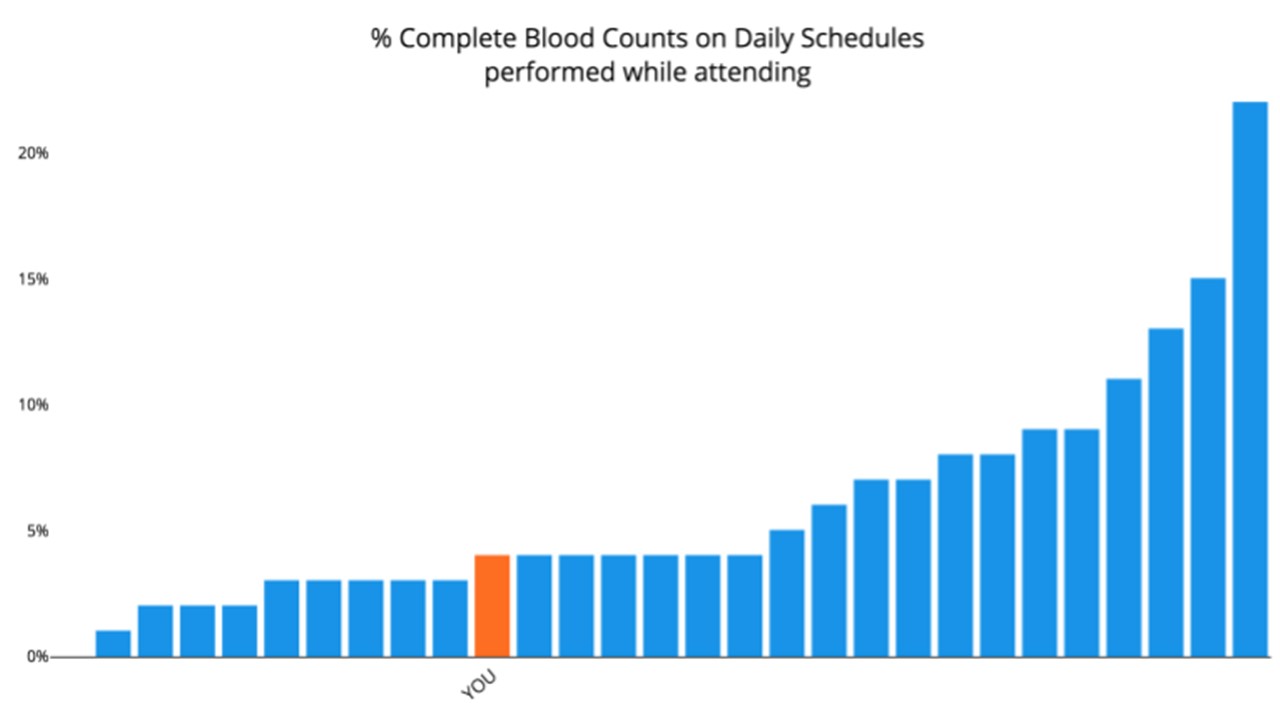
Most physicians followed similar trends in each category, with a positive correlation between the percent of daily labs in each category (r = 0.88).
DELIVERY & CONCLUSIONS
Agathos sent each hospitalist a personalized text message on their orders for blood testing and a link to explore peer compare graphs, reference materials, and relevant cases within the Agathos mobile application. A subset of physicians also participated in small group sessions to review the data and discuss their practices.
We will continue to track hospitalist daily lab ordering practices over the next several months, including personalized follow-ups in the Agathos web application about progress.
As in this case, clinical best practices can change over time due to several factors, including advances in medical knowledge, changes in population health, and economic factors that change the costs and benefits of a given decision. The effectiveness of quality improvement and variation reduction initiatives hinges on a data-driven and user-centric approach:
- pull data from clinical records
- calculate physician metrics with a convincing attribution methodology
- prioritize findings among all other possible insights
- deliver feedback in an engaging, persuasive, respectful way
Curious about your group’s clinical variation? Contact us to request a demo.

About Author
